
Adapting evidence-informed population health interventions for new contexts: a scoping review of current practice | Health Research Policy and Systems

Map of adaptation studies
We identified 298 eligible studies for the map (see Fig. 2). Table 2 shows their characteristics according to the level of intervention. Additional file 4 provides further details regarding the map, including the topic area and focus of the intervention, adaptation context, and types and framework considered in each study. Most studies targeted micro-level interventions (84%), provided a description of adaptation (50%), did not report using adaptation guidance (73%), and described a transfer of an intervention to a new target group within the same country (63%) (most of these were within the United States). Studies covered a range of topic areas, including health behaviour interventions (23.5%), mental health (19%), sexual health (16%), parenting and family-centred interventions (15%), and substance use (10%).

Map of adaptation studies (n = 298). This alluvial plot shows how data are distributed within and across the categories of the map. For example, it shows that health behaviours (darker pink) represent one of the intervention topics and that most of the studies with this topic reported micro-level interventions. Similarly, we can see that most studies adapting an intervention to a new country (dark purple) do not report using any adaptation guidance
Characteristics of selected studies
Overall, 28 studies were selected for in-depth analysis (see Table 3). Since we found only one study describing a macro-level intervention (see Table 2) and no study describing a meso-level intervention, our sampling within these categories yielded 23 studies. To enlarge our sample, we randomly selected an additional five studies from those describing the transfer of an intervention to a new country, because one of the gaps in the existing guidance papers on adaptation was that they do not sufficiently address adaptation between countries [5].
The selected studies focused on a range of topics: mental health and parenting (n = 7), sexually transmitted diseases (n = 6), tobacco and substance use (n = 5), and nutrition and physical activity (n = 5). Seventeen studies were concerned with micro-level interventions, ten with meso-level interventions, and one study with a macro-level intervention. Seven studies provided a description of adaptation, seven evaluated an adapted intervention, and 14 provided both a description and an evaluation. Only six studies reported using a guidance paper as identified in our related systematic review on adaptation guidance. In terms of the contextual change, 12 studies described transferring an intervention into a new country, including both high- and low-and middle-income settings (e.g., transferring an intervention from UK to Australia, from the USA to Pakistan, or from Malawi to Mozambique), and 16 studies described adaptations across different population groups within the same country (e.g., transferring an intervention from general US population to African Americans with lower socio-economic status). The theoretical principles underpinning the adaptation were not often discussed: when reported, these included community-based participatory research (CBPR; n = 9), ecological approaches (n = 2), participatory action research (PAR; n = 1), Roger’s diffusion of innovation theory (n = 1), and the situated-Information Motivation Behavioural Skills Model of Care Initiation and Maintenance (sIMB-CIM; n = 1).
The key themes identified in the selected studies are presented in Fig. 3 and discussed below. Examples are summarised in Table 4.
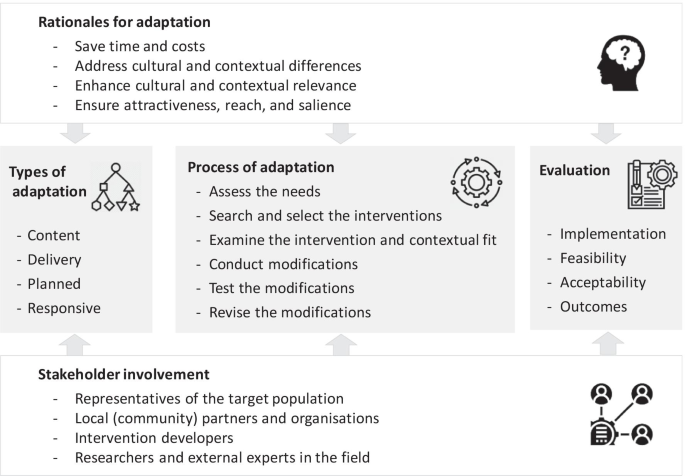
Key themes of adaptation in current practice
Stakeholder involvement in adaptation
As shown in Table 3, a third of the sample of the studies explicitly described their adaptation process as grounded in the principles of CBPR and PAR. These highlight a partnership approach to research with equitable involvement of community, members of implementing organisations, and researchers in all phases of the research, as well as shared decision-making and joint ownership. Our analysis of the textual data also showed that involvement of different stakeholders in the adaptation process, particularly the local community, was the most frequently reported “strength” of the adaptation process [24,25,26,27,28,29,30,31,32,33,34,35]. Specifically, community engagement was viewed to facilitate the acceptability and compliance with the intervention in the new context, enhance responsiveness to local needs, and increase the likelihood of a sustained programme through empowerment and supporting local capacity and self-sufficiency. As Horn and colleagues reflect in their study describing adaptation of an intervention to reduce tobacco dependence among American Indians:
“CBPR principles fostered sound research and meaningful results among a population historically exploited by research. Beyond the project’s quantitative data, the effort resulted in the development of new and successful partnerships, tobacco-addiction intervention programs (e.g., AI N-O-T), tools and resources tailored to community needs, and a multi-tribal interest in educating the youth and communities about tobacco addiction. The community also gained capacity to address the identified problem with greater self-sufficiency via increased grant-writing skills, evaluation knowledge, tobacco education, and financial resources” [27].
Studies considered different stakeholder groups as important to involve throughout the adaptation process. These included representatives of the target population, local (community) partners and organisations (such as those who would be delivering the intervention in a specific context) [24, 26,27,28,29,30,31, 36,37,38,39,40,41], practitioners [28, 30,31,32,33, 36, 39, 41,42,43] (such as clinicians, health professionals, psychologists), intervention developers [28, 30, 32,33,34,35], and researchers and external experts in the field [28, 30, 32,33,34,35]. Involvement of these different stakeholders was emphasised to a greater or lesser extent in different phases of the adaptation process. For example, representatives of the target group and local community partners were frequently emphasised when exploring the needs of the local community and the unique contextual features, as well as piloting of the adapted intervention and implementation. This ensured that interventions were modified with systematic consideration of key values and experiences. In contrast, the roles of intervention developers and experts were highlighted in providing information about the intervention, its components and theory, and in decisions regarding the specific modifications. This ensured that any changes made did not interfere with what the authors described as the intervention core components. Studies discussed different research methods and activities to involve stakeholders, including interviews, focus groups, surveys, theatre presentations, face-to-face meetings, and conferences.
A few studies also described advisory boards which comprised representatives of these different stakeholder groups overseeing and giving advice during all phases of adaptation [25, 29, 32, 34, 37, 39, 41, 43, 44]. For example, in the study on adaptation of a health behaviour intervention for people with impaired mobility, the 13-member national advisory board consisted of health professionals including rehabilitation physicians and occupational therapists, disability researchers specialising in weight loss, experts in human and organisational development, and representatives of community-based disability organisations [25]. The board oversaw and participated in making planned content modifications to the intervention, and provided ongoing advice on how to address the emergent issues identified during delivery.
Key adaptation terms and concepts used in practice
All studies used adaptation as the main term to denote changes made during intervention transfer to a new context, even though we had used several alternative terms in our search strategy. While studies did not provide definitions for adaptation, in a few instances adaptation was linked with the concept of evidence translation [26, 28, 35]. As noted by one of the studies, translation is a broader term which encompasses processes related to how evidence-informed interventions are adopted and adapted for use within community settings and systems [26]. From this perspective, translation was seen to sit within the broader dissemination umbrella, which also includes implementation, evaluation, and maintenance [26]. Tailoring was sometimes used interchangeably with adaptation. We did not find a study providing a specific definition for this term. Fidelity was another frequently used concept [25, 30,31,32, 34, 36, 39,40,41, 45, 46], and commonly referred to the extent of adherence to the original intervention protocol [32, 34, 39, 45] and its core components (i.e., essential components that make the intervention effective) [30, 31, 41]. Definitions for other concepts were not reported in the studies. For example, the term context was not defined but was broadly used to denote different circumstances, such as a geographical location (e.g., Australia vs sub-Saharan Africa), a cultural setting (e.g., First Nations context), or the geographical scope of an intervention (e.g., local vs global).
Presented rationales for adaptation
Rationales for adaptation were reported in 20 of the 28 studies. In most cases the description was brief and non-specific. In comparison to developing a new intervention in a specific context, adaptation of evidence-informed interventions was perceived to save costs and time related to de novo intervention development. Studies most frequently discussed the aims of adaptation to enhance cultural and contextual relevance [41]. Cultural and contextual insensitivity of an intervention was described as potentially contributing to null or negative intervention impacts and lack of acceptance and adherence to the intervention [37, 43]. In contrast, taking this into account could affect engagement with the intervention, its acceptability, feasibility, and outcomes [24,25,26,27,28, 31,32,33,34,35,36,37,38,39,40,41,42,43, 47]. As summarised in one of the studies,
“Considering interventions are most successful when they are both based on science and culturally relevant (Castro et al., 2004), and considering the resources needed to develop and evaluate a new intervention, neither the exact replication of existing EBIs [evidence-based interventions] nor the development of new, culturally sensitive EBIs offers a sustainable solution. In light of this tension, the systematic, cultural adaptation of EBIs for new target populations and settings presents a way forward” [41].
To ensure cultural relevance and contextual compatibility, studies highlighted the need to consider specific cultural values, beliefs, languages, and traditions (e.g., when adapting an intervention addressing tobacco dependence for Native Americans, for whom tobacco has a special role in spiritual and ceremonial events) [27, 33, 34, 36, 40, 43, 47], as well as unique structural characteristics of a new context, such as organisational capacity, and functional and environmental needs (e.g., when adapting an intervention addressing nutrition and physical activity for Jewish schools with specific dietary, behavioural, and belief systems) [25, 26, 39]. None of the studies provided explicit reflections on how relevant these cultural and structural factors are for intervention mechanisms and how they may interact with intervention mechanisms to affect implementation and outcomes in a new context. Other, less commonly mentioned reasons for adaptation included the need to ensure intervention attractiveness [40], reach [45], and salience [38].
Types of adaptation
Content modifications were the most frequently described type of adaptation in the studies [24,25,26,27,28,29,30,31,32,33,34, 36,37,38,39,40,41,42,43, 45, 47, 48]. This often involved additions, deletions, or modifications of intervention components, such as specific activities and their duration. For example, in the adaptation of a health behaviour intervention designed for a general population to serve people with impaired mobility, Betts and colleagues changed all intervention sessions by revising the content, language, and delivery to make them “disability-friendly”, added a specific session on adaptive cooking, and revised the content of physical activity to explicitly address accessibility issues, such as through inclusion of tailored home-based activities [25]. Studies justified some of these content modifications as a response to profound social values and cultural traditions [27, 32, 37, 40]. Table 4 provides further examples. None of the studies reported on programme theories and how these may be modified during adaptation.
Studies also referred to the modifications made to the language and wording of the intervention [25, 28, 33, 34, 36, 40,41,42,43, 47] and its outward design, such as when interventions involved the use of specific materials [24, 25, 27, 28, 33, 34, 37, 40,41,42,43,44]. Modifications to how interventions are delivered constitute another frequently discussed type of adaptation, including changes to the format of delivery and deliverers [25,26,27, 31, 36, 41, 43, 44, 49, 50] (see Table 4).
It should be noted that studies did not distinguish between adaptations that were initially planned and those that were actually undertaken, or offer any explanation for a possible discrepancy between these. We found only one study which differentiated between planned and responsive adaptations [25]. While planned adaptations included modifications that were agreed upon by the adaptation advisory board prior to intervention implementation (pre-intervention), responsive adaptations included unplanned modifications by the study team in response to emergent issues during the course of intervention delivery (concurrent with implementation). For example, during adaptation of the intervention for people with impaired mobility, additional conference calls were offered in the intervention group to complement the in-person sessions in response to the transportation barriers and declining attendance at the in-person sessions [25].
Process of adaptation
Only six studies reported using existing guidance to inform their adaptation process (see Table 3). Nonetheless, most of the studies describing intervention adaptation (and not an evaluation) reported a structured process consisting of sequential phases and steps or key principles [27, 28, 30,31,32,33,34,35,36, 38, 39, 41, 43, 45, 48]. Four studies that did not report a phased process, still described well-demarcated procedures [24,25,26, 44]. For example, when adapting an evidence-informed intervention to increase sexually transmitted disease (STD) testing among Black and Latino sexual-minority youth, Garbers and colleagues described procedures of formative research (including focus groups with the target group to identify their needs), followed by adaptation of the intervention materials, local implementation, and process and outcome evaluation [44]. Studies varied widely in the number of steps described (ranging from 2 to 20), in the level of detail provided, and in how they assigned specific procedures of adaptation across these steps.
Prior to undertaking modifications, many studies described some preparatory procedures. These commonly included assessment of the needs of the new context (e.g., through targeted literature reviews, stakeholder elicitation interviews, or focus groups) [27, 28, 30,31,32, 38, 39, 41, 43, 44, 48], searches for and selection of appropriate evidence-informed interventions [27, 30, 36, 39, 41, 48], and examination of the intervention, its core components, and contextual fit and misfit [24, 27, 28, 30, 32, 33, 39, 41, 43, 45]. Studies reported various ad hoc procedures for selecting appropriate evidence-informed interventions. These included ranking interventions based on specific criteria, such as reporting of a theory-driven approach, use of specific components, and prior implementation of the intervention in the region [36], and judgements of the fit of the intervention and its theory of change with key behavioural and environmental determinants, cultural features, and implementation resources of the new context [39]. Recommendations received through consultations with experts and/or networks of partners [41] was also one of the reported reasons for selecting an intervention for adaptation, as well as its inclusion in a registry of evidence-informed interventions, such as the Centers for Disease Control (CDC) Compendium of Evidence-Based HIV Behavioural Prevention Interventions [30]. None of the studies provided details on the types and nature of evidence that the original intervention had to have in order to be selected for adaptation.
For the specific steps or procedures of adaptation, studies most frequently reported conducting modifications to the intervention content or delivery [24,25,26,27,28, 31,32,33,34,35,36, 38, 39, 41, 43,44,45, 48], followed by preliminary testing of these modifications, such as in a feasibility study [27, 28, 30, 32,33,34,35,36, 38, 39, 41, 43, 45], and making further revisions based on the testing [24, 25, 30, 33, 34, 38, 41, 43, 44, 48]. Decisions on the specific modifications were frequently reported to happen in consultation with expert or community advisory panels comprising a range of stakeholders (see Table 4).
Evaluation of adapted interventions
Studies did not report using any guidance to inform the evaluation of an adapted intervention.
Selected studies aiming to describe an intervention adaptation rather than its evaluation (n = 7, see Table 3) also described evaluation approaches. They reported process evaluations to inform intervention adaptations [30, 42], or pilot studies to examine the acceptability [31], feasibility of implementation [25, 31], and preliminary effectiveness of the adapted intervention [25, 27, 31]. A few of these, however, referred to a parallel ongoing larger efficacy/effectiveness study to examine the effects of the adapted intervention in the new context [25, 31], or recommended conducting such a study as the next step of evaluation [42].
Selected studies aiming to evaluate an adapted intervention reported conducting pilot, process, and outcome evaluations [24, 28, 32,33,34,35,36,37,38,39,40, 43,44,45,46,47,48,49,50,51,52]. Pilot evaluations were often seen as the first important step in testing the adapted intervention for feasibility (related to implementation, recruitment, and outcome measures), acceptability, and preliminary effectiveness (due to small samples). Process evaluations were reported to provide insights regarding the delivery and implementation of the adapted intervention and fidelity.
The subset of studies conducting an outcome evaluation reported using different designs, such as quasi-experimental and pre-test and post-test comparison designs. None of the studies applied a randomised controlled trial design; however, most studies referred to an associated efficacy/effectiveness trial either to be underway [34, 36, 38, 40, 43] or as a recommended or planned next step [28, 32, 33, 35, 45, 48]. While most studies did not provide explicit justification for the effectiveness trial, one paper explicitly noted the need for an effectiveness evaluation of an adapted intervention in light of the conducted adaptations potentially harming the effective components of the original intervention.
“Best practice is to always evaluate an EBI used in a new setting, however, particularly one that has been adapted. Evaluation of adapted EBIs is recommended, since adaptation may harm the effective elements of an EBI (i.e., core elements). Besides this need for impact evaluation, there is a need to evaluate the feasibility and fidelity of intervention implementation in the new population and setting.” [39].
Hybrid study designs, which simultaneously examine effectiveness outcomes and the implementation process (a term used in North America), was highlighted as an ideal design for the evaluation of an adapted intervention [39, 45]:
“Our pilot study provides the initial evidence for conducting larger studies that would assess the effectiveness, impact, and sustainability of our adapted intervention … A hybrid trial, which investigates both intervention and implementation effectiveness, would be an ideal study design for subsequent research as it would allow for the simultaneous, systematic exploration of both intervention and implementation outcomes” [45].
link




