
Effectiveness of acute myocardial infarction interventions on selected outcomes among community dwelling-older adults: a systematic review and meta-analysis

The initial search found 60,739 articles from 12 databases, and 8,659 articles were the rest after duplicate. Based on the inclusion and exclusion criteria, 11 articles were selected for the final comprehensive review. The PRISMA flow diagram of the information flow during the review process is displayed in Fig. 1.
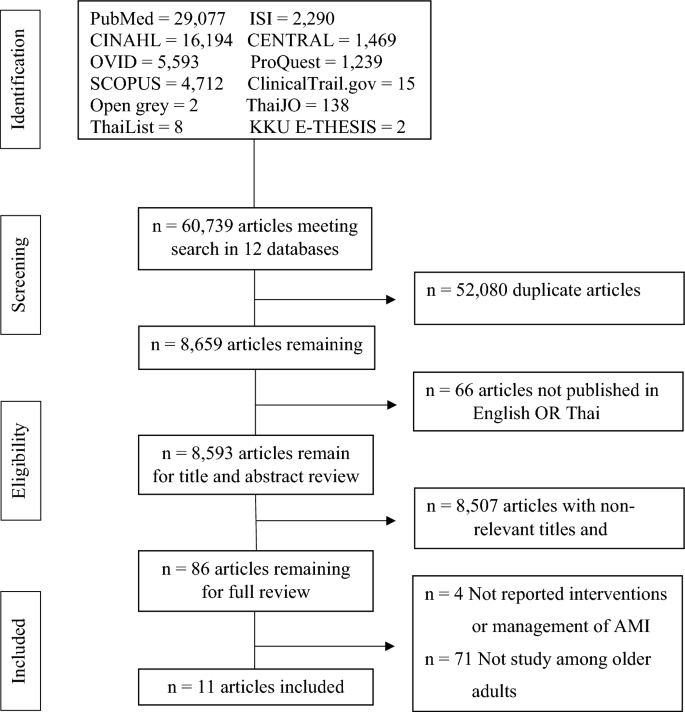
Flow chart of the review process and results.
Characteristics of included studies
Of 11 studies23,24,25,26,27,28,29,30,31,32,33, eight were conducted before 201223,24,25,26,27,28,29,30. Nine studies were in the USA23,24,25,26,27,28,29,30,31, and two were in Germany32,33. Ten studies aimed to explore the effectiveness of intervention/health education on health outcomes24,25,26,27,28,29,30,31,32,33; however, one focused only on elevating the use of emergency services (call 911 or call for emergency medical service: EMS)23. The research designs were nine randomized controlled trials23,24,25,26,27,29,31,32,33 and two quasi-experimental studies28,30. The interventions included a direct mail intervention23, a community-based intervention program24, a Rapid Early Action for Coronary Treatment (REACT) trial25, three Heart Attack Survival Kit23,27,29, two structured/tailored educational/counseling interventions28,30, a Health education-Matters Of Your Heart using the acronym FACTSS & CURB31, and two nurse-based case management for older patients32,33. Five teams used multiple pathways24,26,27,32,33, including face-to-face/home visits, direct mail/telephone, and advertisement. The other five teams used only face-to-face/home visits25,28,29,30,31; another used only direct mail/telephone23. Eleven studies reported the selected outcomes based on the inclusion criteria, including knowledge, belief/attitude, calling 911 or EMS, mortality, readmission, appropriate action/taking aspirin, coping behavior/anxiety, awareness, time of delay/seeking, and malnutrition risk. Only three studies reported the quality of instruments (Table 1).
The major conditions of the study were risk people and people with CAD/AMI—nine implemented interventions in the community24,25,27,28,29,30,31,32,33. Seven studies were conducted among 100% of older adults26,27,28,29,30,32,33, and four were mixed age group, of which over 80% was people aged 60 and older23,24,25,31. Eight studies included both sexes23,24,26,27,29,30,32,33, nine included mixed ethnicity23,24,25,27,28,30,31,32,33, and six reported income23,25,26,27,28,30. Their interventions were eight face-to-face/acronym/teaching24,25,26,27,29,31,32,33. Seven studies were conducted for longer than six months23,24,25,27,29,32,33. Nine studies were not prospectively registered protocols23,24,25,26,27,28,29,30,31. Intervention details included essential information to understand AMI, detect symptoms, and prevent delayed treatment; however, nine focused on overall symptoms or physical reactions23,24,25,26,27,28,30,31,33. Seven studies provided enough detailed interventions that researchers or readers could follow the intervention step by step for their practice24,26,28,29,30,32,33. Only three studies reported that they gave incentives to their participants28,29,31. Eight studies did not report activities for their control groups23,24,25,26,27,29,30,31. Six studies measured outcomes two times (pre-posttest)25,28,29,30,31,32,33. The number enrolled in each group ranged between 50 and 226,958 participants. Significant results were found in the knowledge of AMI30, AMI symptoms26,28, risk factors28, perception28,30, functional status33, hand grip33, aspirin taking26,27,29, and the number of calling 91125,26,27,29 (Table 2). Ten studies were level 1.c of evidence23,24,25,26,27,28,29,30,32,33, and critical appraisal ranked 8–12 for RCT (Table 3) and 6–9 for quasi-experimental study (Table 4). Finally, seven studies were graded as high level23,24,25,26,29,30,32 (Table 5).
Systematic review findings
The interventions found in this review were eight, including direct mail, community-based intervention, multi groups health education, innovative methods of using heart attack survival kits and firefighters, tailored educational/counseling intervention, structured education, and counseling intervention, tricked intervention promoting memory and concern, and nurse-based case management. Types of intervention were grouped, and intervention details and content were provided to guide program development and future study. Moreover, how to deliver and implement interventions was also provided for duplicating in future studies if needed.
Direct mail
The first intervention was a direct mail campaign in which a Brochure was mailed every two months. The information brochure provided detailed information on acute myocardial infarction symptoms and treatment in a neutral tone. The emotional message was designed to reduce the emotional response of fear, embarrassment, and bothering that could prevent or delay appropriate health behavior. The suggestion for decision-making was the family member’s responsibility, not part of the patient’s. Unfortunately, Meischke et al. did not provide details of the information or critical message in the brochure; only the concept and principle were found23.
Community-based intervention
A community-based intervention program was used to reduce out-of-hospital delays. The education message focused on chest pain and other ischemic symptoms, with action if symptoms persisted for 15 min or more. Multiple media channels were used to deliver the message to the general public physicians. Moreover, nurses, paramedics, and other healthcare providers helped deliver the message to high-risk groups. This health education program sequentially emphasized different themes, including general awareness of AMI symptoms and the need for rapid action, development of a Heart Attack Survival Plan, AMI in women, variability of AMI symptoms, bystander response to heart attacks, and use of 9–1-1 to reinforce the primary message24.
Multi-component strategies & groups health education
The multi-component strategies and groups of health education started with meeting focus groups of AMI patients, relatives, and health care professionals. This meeting found key points for AMI survival, symptom recognition, and the need to act fast by calling 911. The advice was to call 911 for ambulance transport to the hospital if experiencing symptoms persisted for 15 min or longer. This intervention included four strategies. First community organization, in which health professionals and leaders of their relevant organizations in each community constituted a local advisory group. Second, public education targeted all residents of the intervention communities with an 18-month program that included six themes. There was a general awareness of AMI symptoms and appropriate action, MI survival plan, women and MI, MI symptom recognition, bystander response to MI, and the importance of contacting EMS. Third, professional education included physicians, nurses, rehabilitation staff, ED staff, and ambulance staff. They should deeply understand AMI and prompt response in emergencies. Finally, the physician taught patients with a history of coronary heart disease (CHD) or CHD risk factors25.
The innovation method of using heart attack survival kit & firefighters
The program under the Heart Attack Survival Kit (HASK) project included a heart attack survival kit, red cardboard containing essential information, and a group discussion. A heart attack survival kit contained the following: eye-catching design and adhesive strips for permanent placement in the home; list of the warning signs of AMI; strong recommendation to call 911; strong recommendation to take an aspirin for chest pain; one 325 mg. uncoated adult aspirin, primary step for cardiopulmonary resuscitation (CPR), and space to write in medications/allergies and essential phone numbers. A red cardboard flyer shaped like a door hanger was provided with essential information about AMI and how to act when experiencing AMI. Finally, group discussion issues around cardiac emergencies with seniors in their communities were set26,27,29. This innovation program, delivered face-to-face by local firefighters, is designed to increase the utilization of 911 and self-administration of aspirin for seniors experiencing chest pain.
The step-by-step program started with passive-consent letters mailed to the homes of all eligible people in intervention areas (24,582 homes), indicating that a local firefighter would personally deliver a HASK soon unless the participant indicated on a self-addressed postcard that such a visit was not welcomed; the eligible individuals returned the postcard. Two weeks after the passive-consent letters were mailed, local firefighters delivered the kits to the homes of the remaining seniors in King County, Washington. More than 300 local firefighters were trained face-to-face by the staff of this study to discuss the contents of the HASK and to assess and respond to barriers to calling 911 and taking aspirin for chest pain29.
Tailored educational/counseling intervention
The Tailored educational/counseling intervention included essential information about the pathophysiology of AMI, Symptoms of AMI, the importance of quick responding, appropriate action in AMI situations, a rehearsal plan, and take-home questions. For the step-by-step intervention, all section was provided: (1) act in time, (2) what is a heart attack?, (3) the importance of rapid treatment of heart attack, (4) the ten most common symptoms of MI, (5) expectation and expected reaction to heart attack, (6) step to survival and rehearsing plan, (7) what factors increase one’s risk? (8) take-home questions28.
Structured education and counseling intervention
The highlights of this intervention were specific details of intervention related to preventive behaviors and delaying treatment in AMI situations and a clear program direction by providing a step-by-step approach. This program included five steps. The first was educational and counseling intervention with details. Second, participants were given educational and counseling intervention, including information about typical and atypical symptoms of AMI, how symptoms may vary, and actions to take in the event of AMI symptoms. An advisory form was given to each participant after the intervention. The form, designed by the NHAAP, listed what the participant may feel if experiencing an evolving AMI, medication instructions, directions to call 911 and ask for an ambulance, and the location of the nearest 24-h emergency department. Participants who received the intervention were asked to place the advisory form in a prominent place in their homes. Third, the participants were asked to repeat the information to ensure comprehension. The fourth was that the intervention was delivered in a one-to-one session with the participant and lasted 30 to 60 min, depending on the participant’s interest, questions, and comments. Finally, the participants recruited at the senior center were asked to refrain from discussing the study with others to avoid contamination between groups30.
Tricked intervention promoting memory and concern
One study applied a trick by using abbreviations with keywords to promote female older adult memory and concern. Because female older adults experienced prodromal and atypical/different symptoms of AMI with others, specific symptoms were provided, and acronyms were developed for easy memories. The deliberate misspelling of FACTSS was highlighted for the women to help them remember the long list of warning signs. Prodromal symptoms were FACTSS, which stood for fatigue, anxiety, chest discomfort, tummy (indigestion), shortness of breath, and sleeping difficulties. The MI symptoms were CURB, which represented chest sensation or pain, unusual fatigue, pain radiating back, jaw, or arm pain, and breathing difficulties. The health education matters of your heart using the acronym FACTSS & CURB was applied among female older adults. The program was delivered in the community to groups of women. A script for the researchers to follow provided consistent information to each group. Immediately after the presentation, the subjects took the post-test, the same as the pre-test31.
A nurse-based case management
The nurse-based intervention is complex, combining components from case management and disease management. Case management focuses on individual care problems of older adults and facility of care coordination; however, disease management pays attention to identifying problems regarding managing AMI symptoms and providing information and individual education. The case-management intervention consisted of a nurse-based follow-up for one year, including home visits and telephone calls. Key elements of the intervention were to detect problems or risks and to give advice regarding a wide range of aspects of disease management, such as symptom management and medication use. A nurse-based case management program includes three steps. First was the initial session, after giving informed consent (so-called “heart book”), followed by home visits. The home visit was arranged 7 to 14 days after discharge, and telephone calls and telephone interviews (at least every three months) were performed. The study nurse assesses the risk level during the first home visit based on compliance, social network, and comorbidities. The higher the risk level, the more contacts (telephone and home visits) were arranged by the study nurse. Finally, the final assessment after 12 months was conducted32. However, another study was a case-management intervention consisting of a nurse-based follow-up for three years. This intervention included home visits and telephone calls. The case-management intervention consisted of a three-year nurse-based follow-up, including home visits and telephone calls, risk management, and symptom management33.
Meta-analysis findings
The meta-analysis showed that people receiving a Kit via home by an Emergency Medical Technician or via direct mail or delivered face-to-face by local firefighters had a higher odd of calling 911 and taking aspirin than those without any intervention (OR 2.55, 95% CI 1.01–6.44) as shown in Fig. 2. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. Based on publication bias analysis, this figure visually indicates the skewness of the effect sizes observed, as shown in Fig. 3. In addition, the left-sided test for funnel plot asymmetry using Egger’s regression test was significant (p = 0.043), supporting the conclusion that significant publication bias was present.

Forest plot for the odd ratios of calling 911 and taking aspirin among AMI patients with and without an intervention: The midpoint of each line illustrates the odds ratio; the horizontal line indicates the confidence interval, and the diamond shows the pooled odds ratio. The red and gray vertical lines indicate the overall effect-size and null-effect values, respectively.

Funnel plot of effect sizes included in the meta-analyses for calling 911 and taking aspirin among AMI patients with and without intervention.
The meta-analysis showed no association between people receiving home-based and nurse-based interventions and those without any intervention regarding time to first unplanned readmission or death (HR 0.94, 95% CI 0.77–1.11), as shown in Fig. 4. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. Based on publication bias analysis, this figure provides no visual indication of the skewness of the effect sizes observed, as shown in Fig. 5. The left-sided test for funnel plot asymmetry using Egger’s regression test was non-significant (p = 0.604), supporting the conclusion that non-significant publication bias was present.

Forest plot for the hazard ratios of affecting time to first unplanned readmission or death among AMI patients with and without an intervention: The midpoint of each line illustrates the hazard ratio; the horizontal line indicates the confidence interval, and the diamond shows the pooled hazard ratio. The red and gray vertical lines indicate the overall effect-size and null-effect values, respectively.

Funnel plot of effect sizes included in the meta-analyses for affecting time to first unplanned readmission or death among AMI patients with and without intervention.
Finally, the meta-analysis showed no association between people receiving community-based and direct mail intervention and those without any intervention regarding delay time to ER (Standardized mean difference = 0.21, 95% CI − 0.20 to 0.62), as shown in Fig. 6. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. Based on publication bias analysis, this figure visually indicates the skewness of the effect sizes observed, as shown in Fig. 7. The left-sided test for funnel plot asymmetry using Egger’s regression test was non-significant (p = 0.441), supporting the conclusion that no significant publication bias was present.

Forest plot for the standardized mean difference of time delay to ER among AMI patients with and without an intervention: The midpoint of each line illustrates the mean difference; the horizontal line indicates the confidence interval, and the diamond shows the pooled mean difference. The red and gray vertical lines indicate the overall effect-size and null-effect values, respectively.

Funnel plot of effect sizes included in the meta-analyses for time delay time to ER among AMI patients with and without intervention.
link




