
Do professionalism, leadership, and resilience combine for professional identity formation? Evidence from confirmatory factor analysis

Introduction
It has been proposed that professional identity formation (PIF) should be a central focus of medical education and this recommendation has been supported by several researchers (1–3). Professional identity formation can be defined as “A representation of self, achieved in stages over time during which the characteristics, values, and norms of the medical profession are internalized, resulting in an individual thinking, acting, and feeling like a physician” (1). University programs can have a significant impact on PIF, in that they are important contributors to the formation of professional identity in medical students (4–6). It has been suggested that the PIF of future physicians is strongly influenced by PIF curricula and pedagogic strategies (7). Curricula should provide adequate opportunity for a student to reconsider their own values and beliefs, by relating to the behaviors that are expected by the medical profession, colleagues, and patients (8). Strategies such as incorporating process-based outcomes along with guided self-assessment have been suggested as potential effective methods to integrate PIF into curricula (9). In terms of educational strategies, several methods have been reported to be effective in PIF. Namely, the importance of role models and mentors, early exposure to patients and the clinical environment, structured feedback, and narrative reflection (10–14). Experiences during clinical teaching have been identified as being particularly important contributors to the student’s formation of their professional identity (15). Similarly the importance of mentorship and clinical placement experience has been proposed as an important factors in fostering resilience and professionalism and leadership skills in medical students (16–18). It has been reported that during longitudinal integrated clerkships, where students participate in the comprehensive care of patients over time, the responsibility students assume as they become co-providers of patient care contributes significantly to their professional identity through the development of meaningful interpersonal relationships along with belonging to a community of practice (19). It has also been suggested if there a lack of professional identity development during training it could result in a loss of trained students from their respective industry (20). The concept of PIF in medicine is not new (21) and much of the existing literature concentrates on what PIF is and why it is important (22). PIF is considered to be of equal importance to the acquisition of clinical knowledge and skills (23). Furthermore, there is an ample amount of research outlining how PIF is developed and is based on multiple theoretical perspectives including developmental and social psychology theory (1–3, 7, 12, 24).
The concept of PIF is complex, multi-factorial, and has been identified to have multiple domains (11, 25). There has been some valid debate in the literature about the difficulty of objectively assessing PIF due to it being a private individual experience (26), however, it has been suggested that if PIF is to be a significant educational objective, robust assessment or markers of its development should be established (23, 27). Furthermore, a systematic review of the literature concluded that there is a dearth of studies which examine the psychometric validity of professional identity measures suggesting that further psychometric validation of quantitative PIF assessments, or its subcomponents, is warranted (5).
In the area of medical education professionalism has been demonstrated to be a key contributor to PIF (11). Traditionally, a summative assessment of professional behaviors has been used as a surrogate for PIF (27). This may be assessed through the completion of professionalism surveys and reflective assignments (28, 29). However, emotional resilience and leadership have also been identified as key elements in forming a personal and professional identity (23, 25, 29, 30). For PIF to occur, medical educators should have a clear understanding of the influences which impact this important developmental process. While multiple other constructs have also been argued to comprise PIF, we deliberately focused on professionalism, leadership and resilience as they are important components in our University’s new Personal and Professional Identity curriculum and investigation into their assessment was required. While literature has linked these factors conceptually and theoretically, it has done so in a qualitative manner, with, to the best of our knowledge, no evidence from quantitative studies. Applying psychometric scaling analysis techniques could allow researchers to delineate quantitatively the interrelationships, if any, among these various constructs, providing support or new insights on these theoretical contentions. Indeed, identifying these interrelationships and the degree to which they may influence PIF could provide significant information for the development of educational strategies for PIF. Our group has recently proposed a quantitative progress assessment of PIF, including professionalism, leadership and resilience (22), and a latent variable analysis of this dataset, therefore, provides a unique opportunity to ascertain whether these constructs do indeed contribute to PIF development. Specifically, we can ascertain the most appropriate theoretical model of PIF, for example comparing models where PIF is informed by resilience, leadership and professionalism (a higher-order model), or alternatives where these constructs are separate (a three-factor model), or if these simply indicate an overall single dimension (a saturated model).
Aim
The present study aimed to quantitatively investigate the extent to which PIF is informed by professionalism, leadership, and resilience, using a latent factor analysis approach.
Methods
Study design
The present study reports a quantitative, psychometric evaluation of the factorial structure of PIF in medical students using data obtained from cross-sectional data from the broader PILLAR (Professional Identity Formation, ProfessionaLism, Leadership, And Resilience) study [for further detail see reference (23)]. PILLAR is an online assessment of the entire cohort of pre-clinical medical students at the RCSI University of Medicine and Health Sciences, Dublin, Ireland. A comprehensive online assessment of PIF, professionalism, leadership, and resilience was conducted using a 76-item questionnaire, which comprised four validated scales and additional questions on participant demographics. All items from the original PILLAR assessment were included in this study’s analysis. The PILLAR assessment was embedded as a compulsory part of the professionalism curriculum in pre-clinical year modules. Although compulsory, students provided voluntary, explicit, and written informed consent if they agreed to their data being used for research purposes. Ethical approval was obtained from the RCSI Research Ethics Committee before conducting the study (REC202005016). The methodology adheres to the STROBE reporting guidelines (31).
Setting
Assessments were completed online by pre-clinical medical students at RCSI University of Medicine and Health Sciences, Dublin, Ireland.
Participants
All 1,427 pre-clinical medical students were invited to complete the PILLAR assessment between September 2020 and February 2021, see our methods paper for further information on methodology (23). The recruitment sample comprised all students from Foundation Year (pre-medicine; FY), Years 1–3 of direct-entry undergraduate medicine (DEM), and Years 1–2 of graduate-entry medicine (GEM). Of this sample, 1,311 participants (93% of eligible medical students) consented to their data being used as part of the research.
Variables
The PILLAR assessment comprised four valid and standardized scales examining PIF, professionalism, resilience, and leadership (23).
Professional identity formation
PIF was assessed by the 9-item Professional Self-Identity Questionnaire (PSIQ) (32). The PSIQ measures 9 domains of professional self-identity within health and social care professions including teamwork, communication, patient or client assessment, cultural awareness, ethical awareness, using patient or client records, dealing with emergencies, reflective practice, and teaching. Respondents rated each statement as to how they would currently identify themselves when undertaking each professional activity on a scale from 0 to 6, where 0 represents the first day as a student doctor, and 6 indicates a newly qualified doctor. After the study pilot, an additional item relating to PIF was included in the study protocol; namely, “I feel like a member of the medical profession.” Participants rated this item along a 5-point response scale from “Strongly disagree” to “Strongly agree.”
Professionalism
Professionalism was captured by 25 items from a 27-item measure of perceptions among medical students toward unprofessional behaviors (33). Two items about inappropriate dress (“Women’s dress,” “Men’s dress”) were excluded as they were not deemed suitable for the present cohort. For each statement, participants responded “yes/no” as to whether they observed, participated in, or considered the behavior to be unprofessional. To simplify analysis as per previous research, and to observe parsimony in the attitudinal assessment of professionalism, only the “perception of professionalism” responses were included in the factor analysis (34).
Leadership
The Medical Leadership Competency Framework (35) outlines the leadership competencies expected of practicing clinicians. Participants considered 15 items on personal qualities and working with others and rated each item as 0 “Very little/None of the time,” 1 “Some of the time,” or 2 “A lot of the time.” Scores were averaged for each domain, where higher scores were indicative of greater levels of leadership.
Resilience
Resilience was measured by the Brief Resilience Scale, which comprises six statement items on the perceived ability to cope with stress (36). Items were rated along a 5-point Likert scale from “Strongly Disagree” to “Strongly Agree,” with higher scores indicating higher levels of perceived resilience.
Data sources
The study investigators provided brief presentations to each year of medical students to introduce the PILLAR assessment and invite them to participate in the research study component. The assessment was distributed to students via online SurveyMonkey software, coordinated by the RCSI Quality Enhancement Office (QEO) which acted as an independent data controller. During class time, the QEO sent automated, individualized emails to all eligible students with a link to complete the assessment. Students were also provided with two weekly reminders. The link took participants to an online participant information leaflet and consent form where students either consented or declined for their information to be used for research purposes. The QEO completely anonymized the responses for consenting participants, removing all identifiable data, before transferring the data to the research team.
Bias
We addressed potential non-response, selection, sampling, and attrition bias through our methodology, by having PILLAR as a compulsory assessment for pre-clinical students, thereby ascertaining data from all relevant pre-clinical years. Due to issues with curriculum reform, it was not possible to have PILLAR as a compulsory assessment for the clinical years, although this will be addressed in the future.
Study size
During September 2020 and February 2021, all pre-clinical students completed the assessment and were invited to participate in this study (n = 1,427).
Statistical methods
The hypothesis that PIF is informed by professionalism (Pro), resilience (Res) and leadership (Lead) was examined by conducting a confirmatory factor analysis of a three-factor higher-order model. The hypothesized (measurement) model was examined against two alternatives: a saturated model, which posited that all professionalism, leadership and resilience items loaded directly onto a single PIF construct, as well as a three-factor model, which assessed professionalism, leadership and resilience as three independent constructs that did not load onto a common PIF factor. Analyses were conducted using R (v4.1.2) in R Studio (v2022.02.0, Build 443) (37). Uni-and multivariate normality tests were conducted using MVN (v5.9) (38). Confirmatory factor analysis was conducted using Lavaan (v.06–9), Psych (v2.1.9) and semTools (v0.5–5) packages (39–41). Model estimation used the Maximum Likelihood Method (MLM) with geomin rotation. Reliability was determined as McDonald’s Omega using MBESS (v4.9.2) (42). Data were found to violate the assumption of multivariate normality (see Supplementary Appendix 1), which can result in inflated χ2-values, subsequently causing inflated model fit indices. To insulate χ2 against the deviation from multivariate normality, and to produce robust standard errors and significance values, the robust Maximum Likelihood Method (MLR) was used when estimating model parameters (43). Goodness-of-fit was examined using absolute fit indices [Root Mean Square Error of Approximation (RMSEA) and Standardized Root Mean Square Residual (SRMR)], which are considered to be acceptable at <0.8 and < 0.06, respectively (44) and relative fit indices [Close Fit Index (CFI) and Tucker-Lewis Index (TLI)], which are considered to be acceptable at >0.90 (45). Inspection of modification indices (MIs) suggested that model fit could be improved if the error covariance for a number of items was constraint-free. Specifically, several items on the Professionalism factor were indicated. The suggested unconstrained error covariances were introduced one by one until the remaining MI values were below the 3.84 threshold (46). It was considered that each of the three factors would make relatively independent contributions to the construct of PIF. To assess this, discriminant validity was examined in several ways. First, the average variance extracted (AVE) for each factor was compared to the average shared variance (ASV) among the three factors (47). Then, the square root of the AVE for each factor was examined against respective standardized correlation coefficients with other factors. Multi-group modeling was then used to assess the equivalence of the measurement model across the first three academic years of undergraduate study. Analysis of variance (ANOVA) was used to compare a multi-group configural model, calculating independent factor loadings and intercepts for each year, with a metric invariant model (where factor loadings were fixed across years) and a scalar invariant model (where factor loadings and intercepts were fixed across years). Critical change thresholds were as follows; RMSEA >0.015, SRMR >0.010, CFI/TLI > 0.010 (48).
Results
Participants
A total of 1,427 students were invited to complete the PILLAR assessment, with n = 1,331 (93%) students responding and n = 1,311 (92%) consenting to their data being used for research. The mean age was 22 ± 3.0 years with just over half of the participants being female. In terms of country of origin, the majority of students were from four individual regions/countries, the Middle East (29%), North America (21.3%), Ireland (16.5%), and Malaysia (11.5%), reflecting the diversity of the student population. Further details on descriptive statistics are in our original paper (23).
Outcome data
Main results: factor analysis—hypothesized model
The hypothesized measurement model was estimated [χ2(986) = 3896.34, p < 0.001]. By the aforementioned criteria, absolute fit indices demonstrated acceptable fit: RMSEA (0.052, 90% CI = 0.050–0.054), SRMR (0.050), but relative fit indices were outside of acceptable values: CFI (0.81), TLI (0.80). Leadership demonstrated the largest factor loading onto PIF (0.70), followed by resilience (0.54), then professionalism (0.27). The items that were then constraint freed and their respective bivariate correlation coefficients are presented in Table 1. The revised model was significant [χ2(971) = 2482.09, p < 0.001] and demonstrated improved fit across most indices, with relative fit indices now presenting with acceptable values: RMSEA (0.038, 90% CI = 0.036–0.040), SRMR (0.042), CFI (0.90), TLI (0.90). Reliability analysis using McDonald’s Omega (ω) indicated that each of the three factors was reliable and that factor reliability could not be improved by removing items: professionalism ω = 0.92 (95% CI = 0.920–0.932), resilience ω = 0.83 (95% CI = 0.814–0.842), leadership ω = 0.79 (95% CI = 0.774–0.807). The model schematic and parameter estimates, including path coefficients and error terms, can be seen in Figure 1, while standardized factor loadings, Omega coefficients and average variance extracted (AVE) can be seen in Table 2. Contrary to the unmodified model, Resilience demonstrated the largest factor loading onto PIF (0.70), followed by professionalism (0.45), and then leadership (0.13). Discriminant validity was observed in relation to the three factors, as the AVE was greater than the ASV (47) and the square root of the AVE was greater than the correlation coefficients for all factors (Table 3) (49).
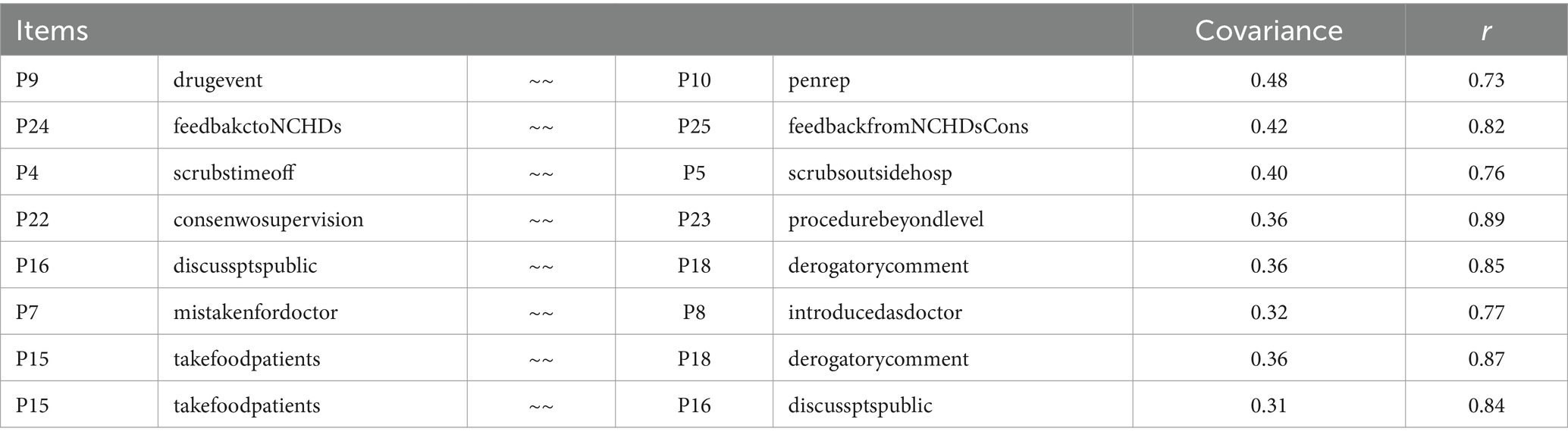
Table 1. Professionalism item covariance and correlations (> 0.07).
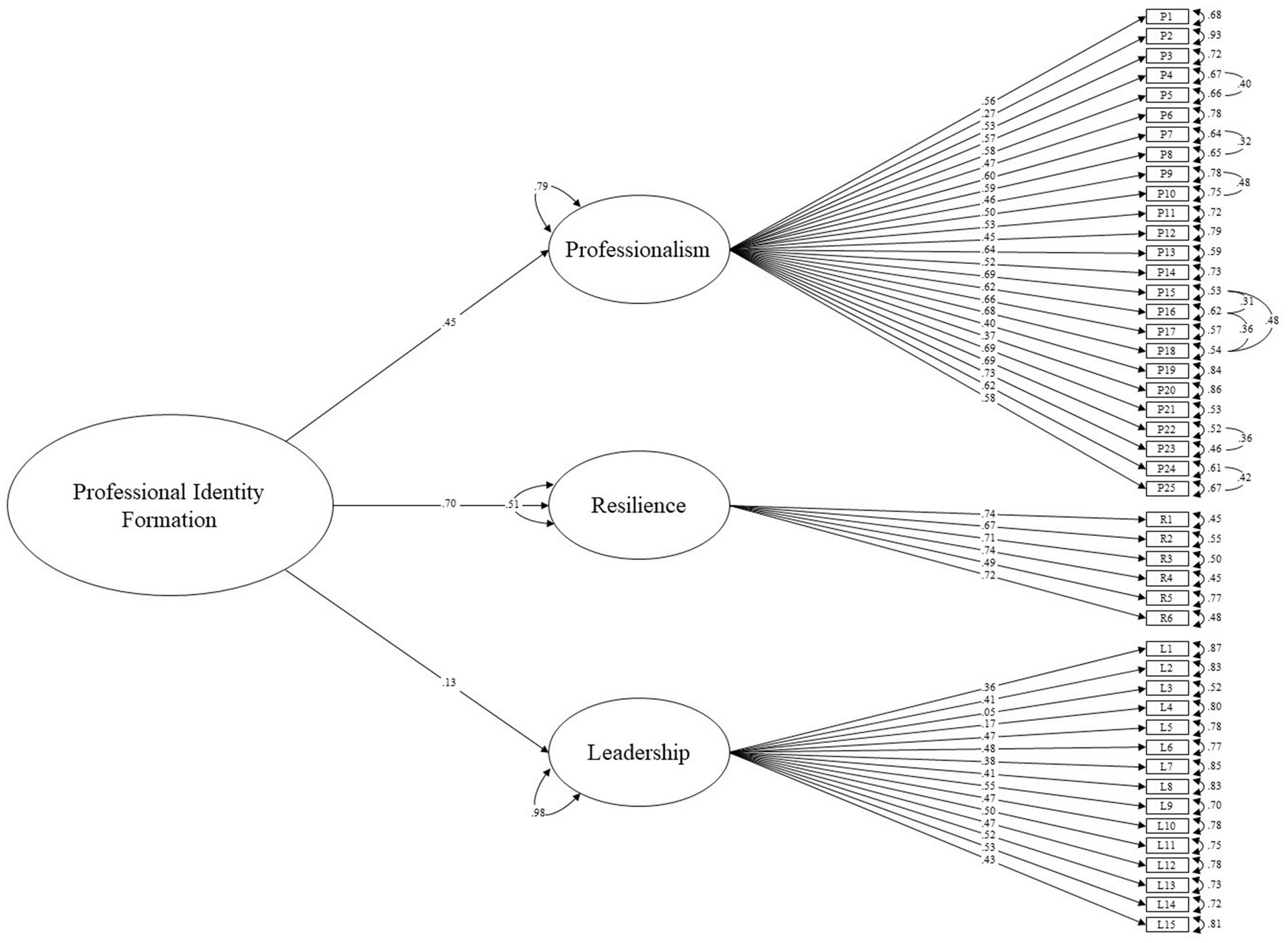
Figure 1. Higher order model of professional identity formation.
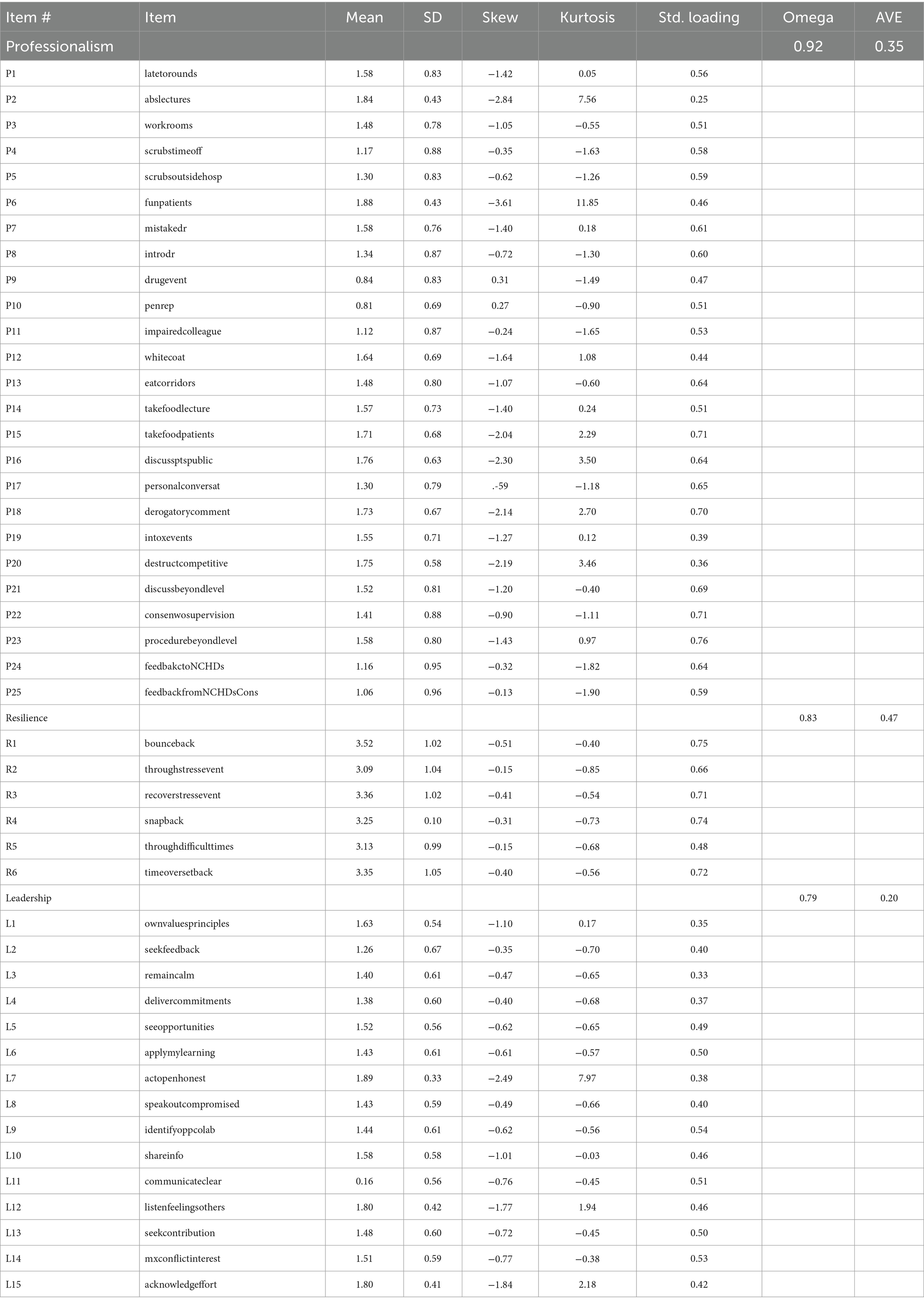
Table 2. Descriptive statistics, item factor loadings, alpha coefficients, and AVE values.
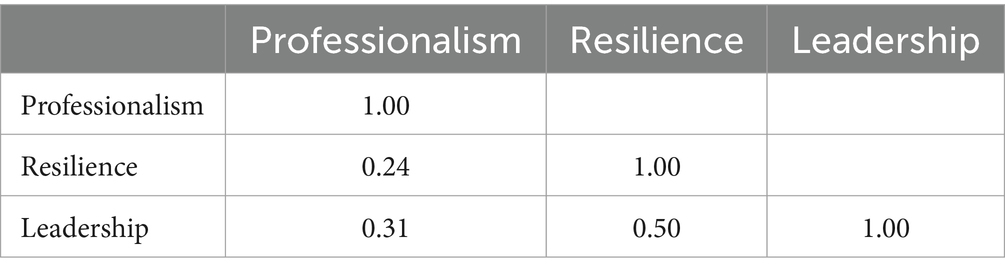
Table 3. Standardized scale correlation coefficients.
Comparison of hypothesized models to alternatives
The hypothesized three-dimensional factor structure of PIF was then compared with an alternative unidimensional (saturated) model using modified indices as per the measurement model, whereby professionalism, resilience and leadership items were allowed to load onto a single PIF factor. A Chi-square difference test was conducted, which indicated that the hypothesized measurement model was a better fit than the alternative model at a significance level of p < 0.001. This was further evidenced when comparing the measurement model fit indices to those of the alternative model 1. The measurement model was also compared against an alternative three-factor model whereby professionalism, resilience and leadership items loaded onto respective factors, but these factors did not load onto a higher-order PIF factor. A Chi-square difference test again indicated that the measurement model presented with a better fit than did alternative model 2 at a significance level of p < 0.001. This was also reflected in the fit indices. The outcomes of the comparisons of the measurement model with the alternative models (see Table 4) provide further support for the hypothesis that professionalism, resilience and leadership are statistically distinct constructs and that these constructs inform a higher-order construct of professional identity formation.
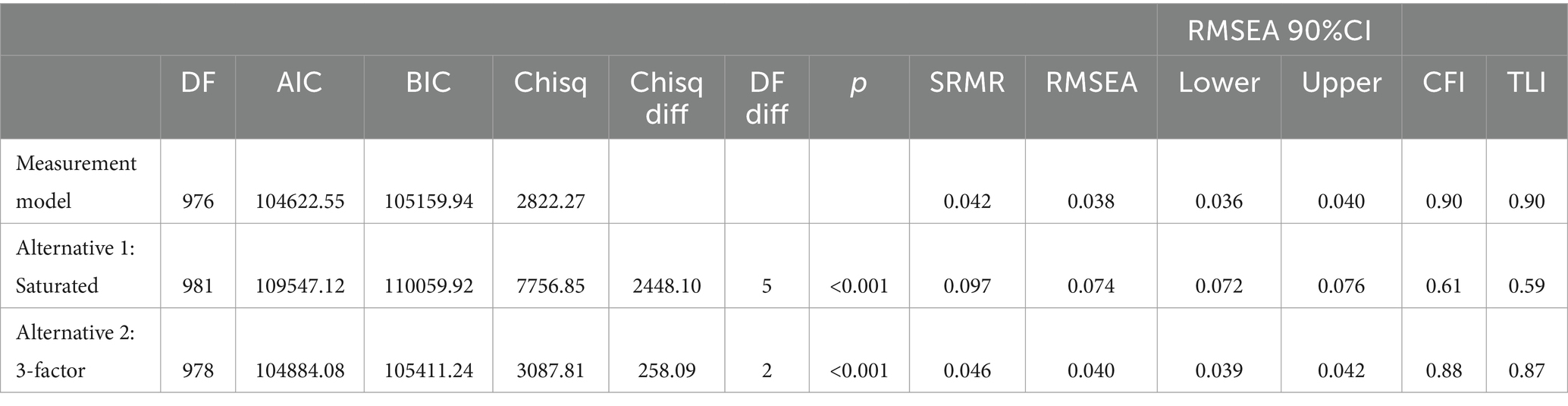
Table 4. Model fit statistics.
Model equivalence across academic year
Multi-group modeling was then conducted to assess the stability of the higher order 3-factor model of PIF over time. Initially, a comparison of fit indices for a configural model with those of both a metric and scalar model suggested little difference in fit across models. This was further assessed using ANOVA, which indicated non-invariance in relation to both the PIF model (metric invariance) and item scoring (scalar invariance) across the three academic years (see Table 5).

Table 5. Invariance analysis by academic year.
Discussion
This paper is the first to conduct and compare factor analytic models of PIF and its contributors. The main findings are that a three-factor higher-order model is the best fit for the data, suggesting that PIF is informed by professionalism, resilience and leadership, which are statistically distinct and account for different aspects of PIF. This higher-order model of PIF outperforms both the saturated model (where all items are allowed to load onto one component) and the three-factor model (where items load on their respective factors, but the factors do not load onto PIF).
Our results provide important quantitative support for the previous qualitative work that suggested PIF is positively influenced by emotional resilience and leadership (25, 29). These results have practical implications for medical education in that they substantiate incorporating professionalism, leadership and resilience into curricula and educational interventions which aim to specifically support PIF. Initially, leadership was found to be the most influential component of PIF, with professionalism being the least influential. However, the professionalism scale required several index modifications to achieve a statistically (while theoretically) sound higher-order PIF model. In the resulting revised measurement model, resilience is presented as the most influential component of PIF, while leadership is presented as the least influential, which are novel and potentially important findings, if replicated. While the models are theoretically identical, the revised measurement model is more statistically sound, as the collinearity issue with the professionalism measure is addressed and the model fit is improved. In light of the required modifications of professionalism and its subsequent impact on PIF loadings, inferences regarding which component of PIF might be most or least influential should be considered inconclusive for now. Future research could aim to explore the respective influences of professionalism, resilience and leadership on PIF with an alternative measure of perceptions of professionalism.
The results of invariance analyses indicated that both the higher-order model of PIF and participants’ perceptions of PIF may change over time. The relatively small difference in Chi-square and fit indices between the configural and metric models suggests that it may be possible to obtain a PIF model that is invariant across the three academic years. Therefore, formal curricular input may be needed to modify these perceptions. Considering the performance of the professionalism scale, it may be best to further examine this with an alternative measure of perceptions of professionalism. As students progress through their undergraduate studies, it is plausible that curricular input and environmental factors might augment perceptions of PIF, or that hidden curricula may indeed subvert or otherwise confound efforts to promote PIF over time (50). This could inform differences in item scores across academic years, resulting in the noted scalar invariance (51).
Although there were some issues with the professionalism measure, the results of this analysis support the viability of a 3-factor higher-order model of PIF, comprising professionalism, resilience and leadership. If these results are replicated in the future, it would compound the suggestion that investing in training in each of these aspects would be core to appropriate PIF formation in future physicians.
Limitations and future research
The major limitation of this paper is the lack of data from students in their clinical years. This will be addressed in future work, as the PILLAR assessment is longitudinal and future cohorts will continue to complete it into the clinical years in a reformed curriculum. The data are cross-sectional only, and future longitudinal work may show different results. Our regression analysis demonstrated significant differences among years on certain variables, however, there was no clear evidence of increasing or decreasing scores by year. Our results point to potential cohort effects and that each class should be taken on its own merits, rather than necessarily expecting a gradient of results from cross-sectional data. However, this result may point to a lack of sensitivity to change in these instruments, which contrasts with other work on the use of essays which do show change over time (52). Future iterations of PILLAR, with longitudinal data for each student, will shed light on these issues. Another potential limitation can be noted in relation to the professionalism measure. The loading for professionalism was initially small. Inspection of modification indices suggested that the overall model fit could be improved by freeing several error covariances. The terms that were freed all pertained to the professionalism factor, which subsequently increased its loading onto PIF. However, this had a detrimental effect on the loading for leadership. In light of what appears to be a significant collinearity issue across several pairs of items on the professionalism scale, it may be that this measure is inadequate. In this regard, it is also instructive to consider that modifying these indices may have affected invariances outcomes (53), thus our conclusions about the relative contributions of each factor to PIF are tentative. Although the higher-order model of PIF as constituting professionalism, resilience and leadership still demonstrated adequate fit, further research could usefully explore the potential for a more optimal and parsimonious higher-order PIF model using an alternative measure of perceptions of professionalism [e.g., the Professionalism Assessment Scale (PAS)] that may not require modified indices (54).
Additionally, while the sample obtained can be considered representative of undergraduate medical students (covering 3 years and two entry pathways), findings might not reflect other types of students, or indeed other types of professions. Further research could be undertaken to examine if the 3-factor higher-order model of PIF might be evident among different types of undergraduate students, for example, those studying engineering, accounting or computer science. It may also be useful to explore if the higher-order model is found among students of other universities. Research could also examine if this model remains stable as students enter into medical professions, and could explore other professions, such as consultancy, law or fast-moving consumer goods.
To conclude, our study is the first to quantitatively support the contribution of professionalism, resilience, and leadership to the development of professional identity, and to delineate the inter-relationships between PIF and these constructs. This information can be used by medical educators when designing curricula and educational strategies intended to enhance PIF. Future work should seek to assess the influence of these constructs longitudinally.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The data that support the findings of this study are available from the corresponding author but restrictions apply to the availability of these data, which were used with permission for the current study, and so are not publicly available. Data is however available from the authors upon reasonable request and with permission of RCSI Research Ethics Committee. Requests to access these datasets should be directed to [email protected].
Ethics statement
The studies involving humans were approved by the Royal College of Surgeons in Ireland Research Ethics Committee (REC202005016). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AR: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. CM: Conceptualization, Investigation, Visualization, Writing – original draft, Writing – review & editing. DB: Conceptualization, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. AH: Conceptualization, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. DH: Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. FB: Formal analysis, Methodology, Validation, Writing – original draft, Writing – review & editing. SG: Validation, Visualization, Writing – original draft, Writing – review & editing. AB: Validation, Visualization, Writing – original draft, Writing – review & editing. FD: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. AR and DH were supported by the RCSI and the Bons Secours Health System. The Bons Secours Health System had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
The authors would like to acknowledge all our student participants in the PILLAR study along with the RSCI Quality Enhancement Office who acted as independent data controllers.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at:
Footnotes
References
1. Cruess, R, Cruess, S, Boudreau, J, Snell, L, and Steinert, Y. Reframing medical education to support professional identity formation. Acad Med. (2014) 89:1446–51. doi: 10.1097/ACM.0000000000000427
PubMed Abstract | Crossref Full Text | Google Scholar
2. Jarvis-Selinger, S, Pratt, DD, and Regehr, G. Competency is not enough: integrating identity formation into the medical education discourse. Acad Med. (2012) 87:1185–90. doi: 10.1097/ACM.0b013e3182604968
Crossref Full Text | Google Scholar
3. Frost, HD, and Regehr, G. “I am a doctor”: negotiating the discourses of standardization and diversity in professional identity construction. Acad Med. (2013) 88:1570–7. doi: 10.1097/ACM.0b013e3182a34b05
Crossref Full Text | Google Scholar
4. de Lasson, L, Just, E, Stegeager, N, and Malling, B. Professional identity formation in the transition from medical school to working life: a qualitative study of group-coaching courses for junior doctors. BMC Med Educ. (2016) 16:165. doi: 10.1186/s12909-016-0684-3
PubMed Abstract | Crossref Full Text | Google Scholar
5. Matthews, J, Bialocerkowski, A, and Molineux, M. Professional identity measures for student health professionals – a systematic review of psychometric properties. BMC Med Educ. (2019) 19:308. doi: 10.1186/s12909-019-1660-5
PubMed Abstract | Crossref Full Text | Google Scholar
6. Cruess, SR, and Cruess, RL. Teaching professionalism – why, what and how. Facts Views Vis Obgyn. (2012) 4:259–65.
PubMed Abstract | Google Scholar
7. Mount, GR, Kahlke, R, Melton, J, and Varpio, L. A critical review of professional identity formation interventions in medical education. Acad Med. (2022) 97:S96–s106. doi: 10.1097/ACM.0000000000004904
PubMed Abstract | Crossref Full Text | Google Scholar
9. Sternszus, R, Slattery, NK, Cruess, RL, ten Cate, O, Hamstra, SJ, and Steinert, Y. Contradictions and opportunities: reconciling professional identity formation and competency-based medical education. Perspect Med Educ. (2023) 12:507–16. doi: 10.5334/pme.1027
Crossref Full Text | Google Scholar
10. Goldie, J
. The formation of professional identity in medical students: considerations for educators. Med Teach. (2012) 34:e641–8. doi: 10.3109/0142159X.2012.687476
Crossref Full Text | Google Scholar
11. Holden, M, Buck, E, Clark, M, Szauter, K, and Trumble, J. Professional identity formation in medical education: the convergence of multiple domains. HEC Forum. (2012) 24:245–55. doi: 10.1007/s10730-012-9197-6
PubMed Abstract | Crossref Full Text | Google Scholar
12. Cruess, RL, Cruess, SR, Boudreau, JD, Snell, L, and Steinert, Y. A schematic representation of the professional identity formation and socialization of medical students and residents: a guide for medical educators. Acad Med. (2015) 90:718–25. doi: 10.1097/ACM.0000000000000700
PubMed Abstract | Crossref Full Text | Google Scholar
13. Cohen, MJ, Kay, A, Youakim, JM, and Balaicuis, JM. Identity transformation in medical students. Am J Psychoanal. (2009) 69:43–52. doi: 10.1057/ajp.2008.38
Crossref Full Text | Google Scholar
15. McGurgan, P, Calvert, KL, Narula, K, Celenza, A, Nathan, EA, and Jorm, C. Medical students’ opinions on professional behaviours: the professionalism of medical students’ (PoMS) study. Med Teach. (2020) 42:340–50. doi: 10.1080/0142159X.2019.1687862
PubMed Abstract | Crossref Full Text | Google Scholar
17. Quince, T, Abbas, M, Murugesu, S, Crawley, F, Hyde, S, Wood, D, et al. Leadership and management in the undergraduate medical curriculum: a qualitative study of students’ attitudes and opinions at one UK medical school. BMJ Open. (2014) 4:e005353. doi: 10.1136/bmjopen-2014-005353
PubMed Abstract | Crossref Full Text | Google Scholar
18. Farquhar, J, Kamei, R, and Vidyarthi, A. Strategies for enhancing medical student resilience: student and faculty member perspectives. Int J Med Educ. (2018) 9:1–6. doi: 10.5116/ijme.5a46.1ccc
PubMed Abstract | Crossref Full Text | Google Scholar
19. Brown, MEL, Whybrow, P, Kirwan, G, and Finn, GM. Professional identity formation within longitudinal integrated clerkships: a scoping review. Med Educ. (2021) 55:912–24. doi: 10.1111/medu.14461
PubMed Abstract | Crossref Full Text | Google Scholar
20. Chin, D, Phillips, Y, Woo, M, Clemans, A, and Yeong, P. Key components that contribute to professional identity development in internships for Singapore’s tertiary institutions: a systematic review. Asian J Scholars Teach Learn. (2020) 10:89–113.
Google Scholar
21. Sternszus, R, Boudreau, JD, Cruess, RL, Cruess, SR, Macdonald, ME, and Steinert, Y. Clinical Teachers’ perceptions of their role in professional identity formation. Acad Med. (2020) 95:1594–9. doi: 10.1097/ACM.0000000000003369
PubMed Abstract | Crossref Full Text | Google Scholar
22. Orsmond, P, McMillan, H, and Zvauya, R. It’s how we practice that matters: professional identity formation and legitimate peripheral participation in medical students: a qualitative study. BMC Med Educ. (2022) 22:91. doi: 10.1186/s12909-022-03107-1
PubMed Abstract | Crossref Full Text | Google Scholar
23. Ryan, A, Hickey, A, Harkin, D, Boland, F, Collins, ME, and Doyle, F. Professional identity formation, professionalism, leadership and resilience (PILLAR) in medical students: methodology and early results. J Med Educat Curri Develop. (2023) 10:23821205231198921. doi: 10.1177/23821205231198921
PubMed Abstract | Crossref Full Text | Google Scholar
24. Weaver, R, Peters, K, Koch, J, and Wilson, I. ‘Part of the team’: professional identity and social exclusivity in medical students. Med Educ. (2011) 45:1220–9. doi: 10.1111/j.1365-2923.2011.04046.x
PubMed Abstract | Crossref Full Text | Google Scholar
26. Veen, M, Skelton, J, and de la Croix, A. Knowledge, skills and beetles: respecting the privacy of private experiences in medical education. Perspect Med Educ. (2020) 9:111–6. doi: 10.1007/S40037-020-00565-5
PubMed Abstract | Crossref Full Text | Google Scholar
27. Cruess, S, Cruess, R, and Steinert, Y. Supporting the development of a professional identity: general principles. Med Teach. (2019) 41:641–9. doi: 10.1080/0142159X.2018.1536260
PubMed Abstract | Crossref Full Text | Google Scholar
28. Kalet, A, Buckvar-Keltz, L, Harnik, V, Monson, V, Hubbard, S, Crowe, R, et al. Measuring professional identity formation early in medical school. Med Teach. (2017) 39:255–61. doi: 10.1080/0142159X.2017.1270437
Crossref Full Text | Google Scholar
29. Wald, HS, White, J, Reis, SP, Esquibel, AY, and Anthony, D. Grappling with complexity: medical students’ reflective writings about challenging patient encounters as a window into professional identity formation. Med Teach. (2019) 41:152–60. doi: 10.1080/0142159X.2018.1475727
PubMed Abstract | Crossref Full Text | Google Scholar
31. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, and Vandenbroucke, JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
Crossref Full Text | Google Scholar
32. Crossley, J, and Vivekananda-Schmidt, P. The development and evaluation of a professional self identity questionnaire to measure evolving professional self-identity in health and social care students. Med Teach. (2009) 31:e603–7. doi: 10.3109/01421590903193547
PubMed Abstract | Crossref Full Text | Google Scholar
33. Reddy, ST, Farnan, JM, Yoon, JD, Leo, T, Upadhyay, GA, Humphrey, HJ, et al. Third-year medical students’ participation in and perceptions of unprofessional behaviors. Acad Med. (2007) 82:S35–9. doi: 10.1097/ACM.0b013e3181405e1c
PubMed Abstract | Crossref Full Text | Google Scholar
35. NHS Leadership Academy. Medical leadership competency framework: self-assessment tool. United Kingdom: NHS Institute for Innovation and Improvement (2012).
Google Scholar
36. Smith, BW, Dalen, J, Wiggins, K, Tooley, E, Christopher, P, and Bernard, J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. (2008) 15:194–200. doi: 10.1080/10705500802222972
PubMed Abstract | Crossref Full Text | Google Scholar
37. Team R Core. R: a language and environment for statistical computing [computer program]. Vienna: R Foundation for Statistical Computing (2013).
Google Scholar
38. Korkmaz, S, Goksuluk, D, and Zararsiz, G. MVN: multivariate normality tests. The R Journal. (2014) 6.
Google Scholar
39. Rosseel, YJT, Rockwood, N, Oberski, D, Byrnes, J, Vanbrabant, L, Savalei, V, et al. The Lavaan tutorial: department of data analysis. Belgium: Ghent University (2023).
Google Scholar
41. Jorgensen, TD PS, Schoemann, AM, Rosseel, Y, Miller, P, Quick, C, Garnier-Villarreal, M, et al. SemTools: useful tools for structural equation modeling. R package version 0.5-6. Available at: (2022).
Google Scholar
43. Cangur, S, and Ercan, I. Comparison of model fit indices used in structural equation modeling under multivariate normality comparison of model fit indices used in structural equation modeling under multivariate normality. J Modern Appl Statist Methods. (2015) 14:152–167. doi: 10.22237/jmasm/1430453580
Crossref Full Text | Google Scholar
44. Lt, H, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
Crossref Full Text | Google Scholar
45. Schermelleh-Engel, K, Moosbrugger, H, and Müller, H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res. (2003) 8:23–74.
Google Scholar
47. Alumran, A, Hou, XY, Sun, J, Yousef, AA, and Hurst, C. Assessing the construct validity and reliability of the parental perception on antibiotics (PAPA) scales. BMC Public Health. (2014) 14:73. doi: 10.1186/1471-2458-14-73
PubMed Abstract | Crossref Full Text | Google Scholar
48. Chen, FF
. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Model Multidiscip J. (2007) 14:464–504. doi: 10.1080/10705510701301834
Crossref Full Text | Google Scholar
49. Fornell, C, and Larcker, DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. (1981) 18:39–50. doi: 10.1177/002224378101800104
Crossref Full Text | Google Scholar
50. Archer, R, Elder, W, Hustedde, C, Milam, A, and Joyce, J. The theory of planned behaviour in medical education: a model for integrating professionalism training. Med Educ. (2008) 42:771–7. doi: 10.1111/j.1365-2923.2008.03130.x
PubMed Abstract | Crossref Full Text | Google Scholar
51. Putnick, DL, and Bornstein, MH. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. (2016) 41:71–90. doi: 10.1016/j.dr.2016.06.004
PubMed Abstract | Crossref Full Text | Google Scholar
52. Kalet, A, Buckvar-Keltz, L, Monson, V, Harnik, V, Hubbard, S, Crowe, R, et al. Professional identity formation in medical school: one measure reflects changes during pre-clerkship training. MedEdPublish. (2016) 7:41. doi: 10.15694/mep.2018.0000041.1
Crossref Full Text | Google Scholar
53. Jorgensen, TD
. Applying permutation tests and multivariate modification indices to Configurally invariant models that need Respecification. Front Psychol. (2017) 8:1455. doi: 10.3389/fpsyg.2017.01455
PubMed Abstract | Crossref Full Text | Google Scholar
54. Klemenc-Ketis, Z, and Vrecko, H. Development and validation of a professionalism assessment scale for medical students. Int J Med Educ. (2014) 5:205–11. doi: 10.5116/ijme.544b.7972
PubMed Abstract | Crossref Full Text | Google Scholar
link




